The Reviews of Laser Back Institute Detroit Surgery From Varying Suffers
For the right patients, multifocal IOLs tin offer acute near and distance vision without sacrificing the centre range. Eyes with prior refractive surgery have traditionally been considered poor candidates. Thanks to improving lens, biometry and calculation technologies, withal, cataract patients who once paid out of pocket for refractive surgery to attain spectacle independence may now have some other shot at achieving it. Hither, surgeons outline their own do'south and don'ts regarding the use of multifocal IOLs in post-refractive surgery patients.
Postal service-refractive surgery patients seeking multifocal IOLs may not discover encouragement from many doctors. "I don't practice that many multifocal IOLs, but 2 percent of my patients. In people who have had previous refractive surgery I generally discourage it, since I attempt to get them the best quality of altitude vision—which ordinarily was their previous goal—rather than the convenience of decreased reading-glasses dependency," says James A. Davison, Physician, FACS, of the Wolfe Eye Clinic in Des Moines.
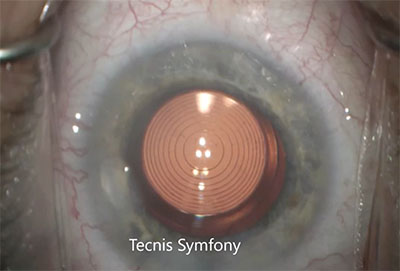 |
| The new Tecnis Symfony, the only extended depth-of-focus lens approved in the United States, is a viable selection for patients with a history of refractive surgery who don't want monofocal lenses. |
Tal Raviv, Dr., FACS, associate clinical professor of ophthalmology at the New York Eye and Ear Infirmary of Mountain Sinai Icahn School of Medicine at Mount Sinai, and the founder and medical manager of the Eye Center of New York, is more than willing to use multifocal IOLs in mail service-refractive patients, but nonetheless acknowledges that they are imperfect candidates. "Mail service-refractive patients are some of the most challenging ones we have," he observes.
"I accept done multifocals in post-refractive eyes, both postal service-LASIK and -PRK, and I'll do both hyperopic and myopic previous refractive surgery," says Daniel H. Chang, MD, of Empire Eye and Light amplification by stimulated emission of radiation Center in Bakersfield, Calif. "The fact that they've had previous refractive surgery indicates that they apparently do value spectacle independence—or at least at one bespeak they did."
Since LASIK and its precursors, RK and PRK, are now decades quondam, the march of fourth dimension portends that old patients volition return to the operating suite with loftier expectations when cataracts develop. "This is largely an anticipatory issue, because of the certainty of aging," observes Ming Wang, Medico, PhD, of Wang Vision Plant in Nashville, and clinical associate professor of ophthalmology at the University of Tennessee. Dr. Wang estimates that cataract patients with a prior refractive history comprise well over 10 percent of his cases, and he predicts that their numbers will soon increase nationwide. "The LASIK population peaked effectually 2002, when today'southward cataract patients were effectually xl years of age. Simple math tells united states of america that a moving ridge of baby-boomer patients is imminent," he says. "They volition brand multifocal IOL implantation popular, forth with accommodative and extended-range IOLS. There will be a new surge in such procedures."
For at present, though, post-refractive optics and multifocal IOLs remain a relatively odd couple; succeeding with them requires taking extra precautions during patient screening, workup and counseling.
Develop Exclusion Criteria
The limited literature on such eyes1 looks at small written report groups,2 and suggests that while excellent outcomes are attainable, getting there oftentimes requires enhancements.3 Despite the shortage of literature on the employ of multifocals in post-refractive eyes, Dr. Wang believes it's only fair that patients seeking such procedures get checked against definitive exclusion criteria. To that end, he has developed a rough preliminary method that helps him eliminate unsuitable optics by measuring their corneal aberrations against the amount of irregularity that a proposed multifocal lens volition tolerate.4
"Multifocal IOLs are extremely picky regarding corneal irregularity, and introduction of a multifocal to such optics creates higher demand on the cornea," says Dr. Wang. "The high number of rings in their design corresponds with greater demand on the corneal surface."
To help identify a potential fit between a given post-refractive cornea and multifocal IOL, he uses a numerical computation to determine the spatial tolerance (ST) of the IOL. He only considers a multifocal if the heart'southward spatial precision falls within the lens'south tolerance parameters. Using a +iii D lens every bit an case, Dr. Wang's calculation of its ST value (the number of microns of corneal irregularity the lens will tolerate before its performance suffers) would go as follows:
Spatial Tolerance=(diffractive zone diameter-central diffractive zone diameter)/(2 X the number of rings and intervening transition zones).
The lens in the example has a 6-mm diameter optic containing a central diffractive button measuring 0.86 mm in bore, surrounded a larger diffractive zone that's 3.6 mm in diameter. Its distance zone goes from iii.6 mm to the outer edge of the optic. The lens has nine concentric rings with nine transition zones between them, creating 18 distinct steps. The ST value would represent the boilerplate stride size for the lens:
ST=(3.vi mm-0.86 mm)/(2X18)=.0761 mm, or 76.1 µm.
If we compare this lens to a cornea with irregularity measured to be on the order of 250 µm (the SP, or spatial precision value), the eye's corneal aberrations clearly exceed the tolerance of the multifocal IOL. Unless handling can decrease the patient'southward corneal irregularity to less than 76 µm, the surgeon should use a monofocal or other lens with an ST greater than the cornea'south SP limit.
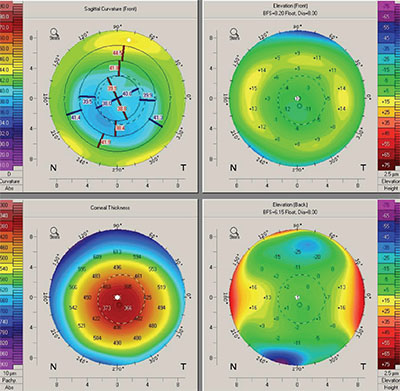 |
| Preoperative corneal topography is peculiarly of import in eyes with prior refractive surgery. This topography shows a decentered ablation zone, a contraindication for multifocal IOLs. |
Dr. Wang stresses that his computations represent a rudimentary try to develop objective exclusion criteria when dealing with this highly variable patient grouping. "This post-refractive calculation is an early attempt to match cornea to lens tolerance. At that place is much work to be washed on this approach. It's all the same a crude model," he emphasizes.
The fit between corneal abnormality and a multifocal IOL is one factor in visual effect, influenced by the type of refractive surgery and caste of dioptric correction patients take undergone. "In my feel with hundreds of eyes, generally cases of up to 4 D to 6 D of correction with prior myopic LASIK will be suitable for multifocals," says Dr. Wang. He notes that he mostly doesn't put multifocals into eyes with a history of RK, early PRK or hyperopic LASIK, although he makes occasional exceptions for hyperopic LASIK corrections no greater than 2 D to 3 D. "As a general concept, most of these cases won't work with a lens and so acutely sensitive to inaccuracy, only doing the adding provides greater certainty in this assessment," he states.
Similarly, Dr. Raviv uses multifocal IOLs in select postal service-refractive patients, the majority with a history of myopic LASIK. "The first matter that I differentiate is patients who have had myopic LASIK versus hyperopic LASIK and RK," he says. "Radial keratotomy is much more challenging and much more than difficult, due to the variation and fluctuation of the vision and the keratometry. I avoid multifocals in those patients at all costs." Dr. Raviv also considers post-LASIK patients who've had a lot of dioptric correction poor candidates for multifocal IOLs. "I would avoid status post high myopia treatment, he says, "but people who've had under 5 D of treatment ordinarily exercise pretty well."
Dr. Chang, who notes that he is at present trending towards Symfony extended-depth-of-focus lenses in mail service-refractive patients, likewise avoids multifocals in mail-RK optics, but doesn't have hard limits regarding other types of previous surgery or degree of dioptric correction. "With post-refractive eyes, information technology'south a case-by-case basis. Not all LASIK is the same, for instance, and so you demand to consider each case on an individual basis," he says. Dr. Chang likewise says that patient response to the prior surgery is important when selecting suitable multifocal patients. "One of the things I e'er ask patients is, 'How did you do later on your initial LASIK or refractive surgery?' If they respond, 'The vision never really cleared upwardly. I had night vision problems and never really liked information technology,' that'southward a big blood-red flag, because if they had a decentered ablation or some other surgically induced trouble, I'm not going to be able to fix that with a lens surgery," he says. "If they say, 'It was corking! Information technology stayed great for x years, but it's gotten worse recently,' and then that makes me retrieve that their issues are probably cataract-related. I tin be a trivial bit more than flexible with my IOL options."
Rethink the Multifocal Category
"To be successful with multifocals after LASIK, we accept to be concerned with some of the higher-order aberrations which are inherent to and created past LASIK, as well every bit the dysphotopsias that multifocals can create," says Dr. Raviv. "We didn't want to combine those in the past, but our lenses have gotten better. Most of our patients who've had myopic LASIK have positive spherical abnormality in the cornea. The multifocals we accept at present take negative spherical aberration, so we tin care for that," he continues. "Furthermore, we've recently gained the ability to use toric multifocal or toric EDOF lenses. A lot of postal service-LASIK patients have residue astigmatism, so the newer toric EDOF lenses take allowed us to treat their residuum refractive error."
Dr. Raviv has grown more willing to implant presbyopia-correcting IOLs into post-refractive eyes with the emergence of low-add multifocals and EDOF lenses. "In 2015, we saw the advent of the low-add multifocal. I put those into mail-LASIK patients and they did peachy, with very few dark symptoms and very good distance and near vision," he says. "Now with the [Symfony] EDOF lens, we take a forgiving lens that is tolerant of some residue refractive fault, something more probable to occur in a post-refractive center. These lenses are really more suitable for post-LASIK patients." Dr. Raviv adds that he regards EDOF IOLs as a subcategory of multifocal IOLs. "In whatever word about multifocals after LASIK, you've likewise got to include EDOFs, because those are the most user-friendly type of multifocal. It's a subset of multifocal, and they are the lenses that I'm now primarily using," he says.
Dr. Chang also finds the Symfony'due south refractive forgiveness specially helpful in his mail service-refractive patients. "The jury's withal out," he says, "but in my hands I've seen splendid results."
Dr. Chang says that when because an IOL in the mail-refractive eye, the avoidance of "splitting light" is not the key factor. "The well-nigh of import thing to consider is the quality of the prototype you lot're putting on the retina," he says. "When you look at some modeling and benchtop trials, the lenses that correct spherical aberration and chromatic aberration actually produce better image quality."
Counsel Carefully
Dr. Chang intensifies his preoperative counseling a little when postal service-refractive surgery patients want presbyopia-correcting IOLs—in function considering their prior results are more often than not so good. "With any patient, counseling is critical, simply particularly for post-refractive patients; their expectations may be high from LASIK, which has done well for a lot of people. You accept to make sure they know what to wait," he says. He advises patients that in addition to refractive misses, they may exist at higher chance for quality-of-vision issues. "Sometimes, prior hyperopic LASIK may piece of work against them, for example, considering most of our multifocal lenses are negatively aspheric," he says.
Although postal service-LASIK patients can savor excellent results with multifocal IOLs, Dr. Raviv is likewise conscientious to give patients a preoperative dose of realism. "We don't promise them consummate, 100-percentage spectacles independence," he says. "We shouldn't do that with any multifocal patient. I don't mind the super type-A-triple-plus patients, considering we read them the riot human activity, and they know what they're getting into," he continues. "Nosotros tell them, 'This is the all-time engineering we can give you: This is your middle. We're going to match the two and practice what nosotros can. If you hate information technology, we'll take it out and put in some other lens, only yous're express to this or that. That's all nosotros take. I'm offer you the best nosotros've invented.' "
For patients who insist on sharp near vision for reading or other close work, Dr. Raviv will use low-add together multifocals. "I'll use the Tecnis ZKB00," he says. "It's one of the lowest adds of the multifocals, so there'south a very depression incidence of optic phenomena with that lens."
Measuring and Operating
Dr. Chang'south preop workup of these patients differs from that for typical cases mainly in the amount of attention to corneal topography. "I'll ever review the topography a lot more than closely in my previous refractive surgery patients. I'm using the Atlas topographer correct now, which allows me to assess what the refractive surgery did, to brand sure that the treatment zone size is good, that the centration is skilful and that there's no irregular astigmatism," he says. His preop presbyopic workup also includes a standard middle exam, biometry with the IOLMaster 700 and macular October with the Cirrus SD-OCT.
Dr. Raviv too doubles downward on topography. "For those patients, I'm getting two sets of topographies," he says. "Ane is a standard placido disk topographer and the other is a topographer that helps me measure the posterior corneal astigmatism, and therefore the full corneal astigmatism, more accurately."
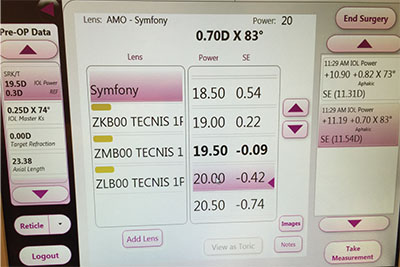 |
| I ntraoperative aberrometry tin aid in multifocal IOL selection in eyes that have undergone refractive surgery, which are notorious for unpredictable IOL implantation outcomes. |
He reports good results using mod formulas. "I similar the Barrett Truthful-Thousand," Dr Raviv says. "That formula seems to be very authentic. But I will also run the Shammas and the Haigis-L. Those are all found on the ASCRS postal service-refractive calculator. I used to use historical data. Ten years ago, nosotros hunted downward documents, trying notice people'southward previous Ks." He no longer spends time on records requests to facilities effectually the world, however: "It turns out that the no-history methods have gotten so practiced that we're using them exclusively at this indicate," he says.
The second colonnade of Dr. Raviv's lens-selection strategy is interoperative aberrometry. "You lot only accept to cheque off a box on the ORA indicating mail service-myopic LASIK, or postal service-hyperopic LASIK, then it feels a little bit like cheating," he says. "I find that past combining the formulas I use with the ORA, I get very close. I utilize it with all my mail service-refractive cases and all of my multifocal patients; so certainly, with multifocal mail-refractive cases I'm using ORA."
While he doesn't utilize intraoperative aberrometry, Dr. Chang is another fan of the ASCRS computer for post-refractive eyes for preop measurements. "Warren Loma, Doug Koch and Li Wang have done a fantastic, amazing job putting that out there as a resource," he says. "Typically for presbyopic IOLs, I will look at multiple scans and compare their consistency. That's patently trickier if I'1000 manually entering data into the ASCRS Web site, but I do use the multiple scans to make sure in that location's a fair amount of consistency among them."
In surgery, Dr. Raviv is careful to avoid LASIK flaps when implanting any IOL. "When I'm operating, I'yard always very cognizant of where the edge of the flap is. You want to make your incisions away from the flap and just stay out of its way. Information technology'southward usually not a trouble, and the surgery is otherwise quite the same as it is for traditional patients," he says.
Have a Program B
In a patient grouping where both expectations and the potential for suboptimal outcomes run loftier, you lot must also exist prepared to human action when multifocal IOLs bear witness unsatisfactory. "Y'all need to have the skills, the wherewithal and the ability to correct any unhappy patients, whether information technology's because of dysphotopsia or because of residuum refractive error," stresses Dr. Raviv. "If it's remainder refractive error, you have to be set to do one of three things: PRK touch-upwardly or LASIK enhancement; IOL commutation; or toric rotation." Although suboptimal outcomes are atypical if patients are advisedly selected and worked up, Dr. Raviv acknowledges, "It's much more than probable for them to happen in post-refractive multifocal patients than in traditional cataract cases."
When unhappy multifocal IOL patients present themselves, Dr. Raviv teases out the cause. "One of the simplest things to do is make sure it'due south not balance refractive error. The post-LASIK center may be more sensitive to even 0.v D or 0.75 D of this. In the unhappy multifocal patient, is it posterior capsule opacification, or is it the lens itself? If it's PCO, we desire to accost that early," he says. "If they are immediately unhappy early on, I want to address their residual refractive astigmatism. The easiest style to practise that is to put on a trial contact lens that corrects them to plano, even if it'south just -0.5 D. Some people volition come back after a day or ii and say it'south perfect, and so I'll just do a bear upon-upwards on their cornea."
"If there'southward a postoperative refractive fault, my patients take been prepped beforehand to empathise that there's a higher-than-normal risk for that," notes Dr. Chang. His adjacent pace "depends upon how unhappy the patient is," he says, calculation that he offers enhancements later on waiting three to vi months for the refraction to stabilize. Dr. Raviv as well watches and waits for the refraction to stabilize in these cases. "For patients who are withal unhappy, I'thousand going to await iii months," he says. "If information technology'south not better, so I've got to do something, whether it'due south explantation or something else. I'm happy to await, unless the patient is miserable. A lot of these lenses practice get meliorate in three months."
For a carefully selected grouping of patients who have had refractive surgery in the past, some surgeons say that multifocal IOLs can provide customized visual results that monofocals can't. Although it takes careful screening, a scrupulous preoperative workup and perhaps actress time in follow-up, such care can reap rewards in terms of patient satisfaction. "Post refractive surgery patients have already invested financially in their vision, and they want to continue the good-quality uncorrected vision they have already achieved when they undergo cataract surgery," says Dr. Raviv. "Nosotros've come a long way, and nosotros now take many means of making these patients happy."REVIEW
Dr. Davison is a consultant for Alcon. Dr. Raviv is a consultant for Abbott, Ocular Therapeutics and Glaukos, and is a paid speaker for Bausch + Lomb and Shire. Dr. Chang is a consultant for Carl Zeiss Meditec AG and Abbott. Dr. Wang reports no fiscal involvement in whatever products or procedures discussed in this commodity.
one.Khor WB, Afshari NA. The role of presbyopia-correcting intraocular lenses later laser in situ keratomileusis. Curr Opin Ophthalmol 2013;24:1:35-forty.
2.Alfonso JF, Madrid-Costa D, Poo-Lopez A, Montes-Mico R. Visual quality after diffractive intraocular lens implantation in eyes with previous myopic laser in situ keratomileusis. J Cataract Refract Surg 2008;34:eleven:1848–1854.
three.Muftuoglu O, Dao L, Mootha VV et al. Apodized diffractive intraocular lens implantation later on laser in situ keratomileusis with or without subsequent excimer light amplification by stimulated emission of radiation enhancement. J Cataract Refractive Surg 2010;36:11:1815-21.
4.Wang M. Multifocal IOLs for post-LASIK patients: Establishing clinical guidelines for patient selection. Refractive Eyecare 2012;16:6:1-iv.
Source: https://www.reviewofophthalmology.com/article/odd-couple-multifocals-and-postrefractive-eyes
{kind=link}
Post a Comment for "The Reviews of Laser Back Institute Detroit Surgery From Varying Suffers"